
Knee Replacement - Partial and Total Knee
-
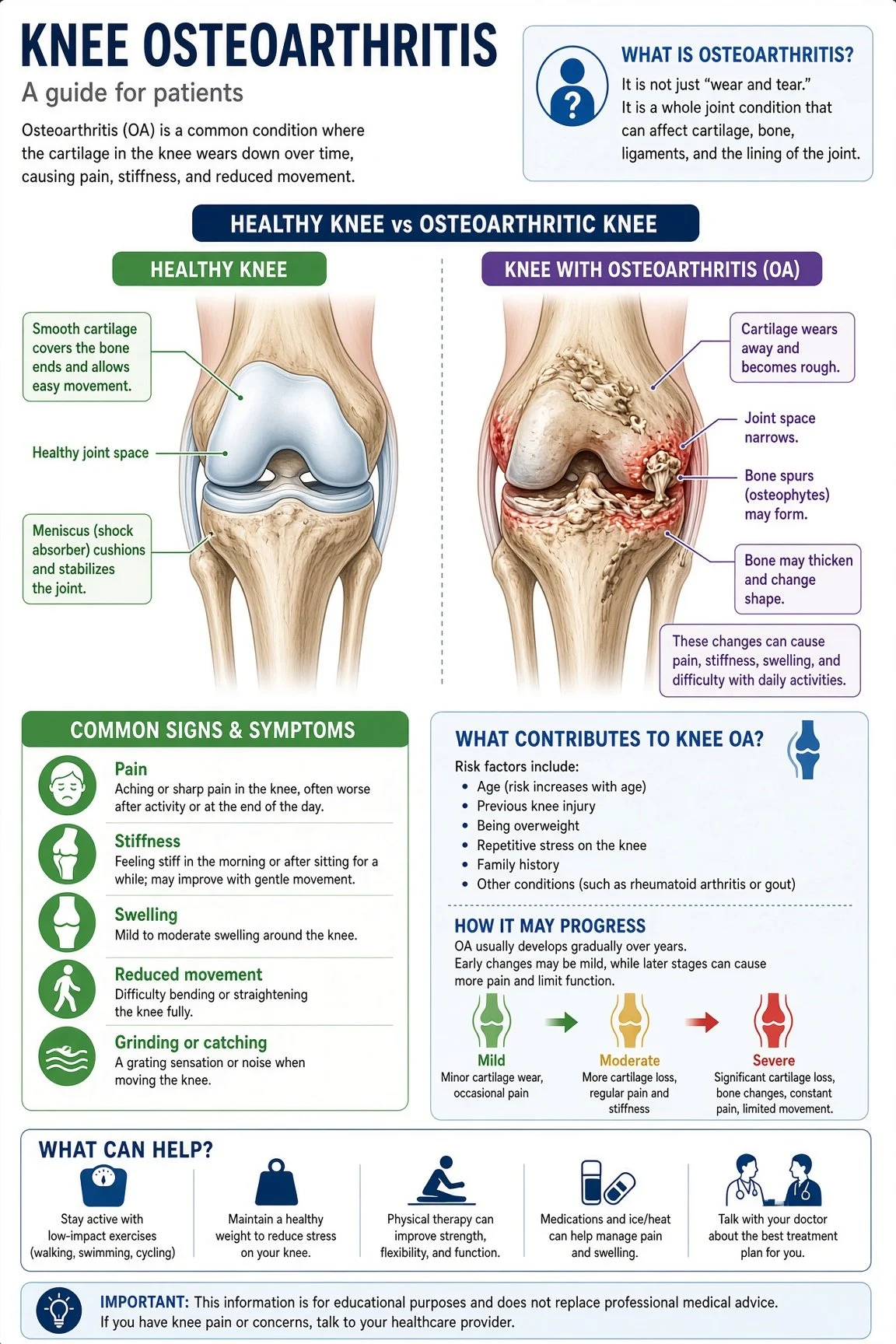
Every joint in the human body comprises two bones that articulate, facilitating movement. To enable smooth gliding of the bones, a thin layer of cartilage is present on top of each bone. This cartilage layer is only a few millimeters thick. An analogy often used is that of icing on a cake, where the icing represents the cartilage and the cake represents the bone. The cartilage is exceptionally smooth, allowing the joints to glide on one another with minimal friction. However, as individuals age or sustain injuries, the thin layer of cartilage gradually diminishes, exposing the bone beneath. This condition is known as arthritis, characterized by the loss of cartilage that exposes the bone underneath. The bone, with its rough surface akin to sandpaper, generates significant friction when the smooth cartilage layer is absent. Consequently, this friction leads to inflammation and pain.
Once cartilage is lost, the body lacks the ability to regenerate it. Cartilage is acellular, meaning it lacks cells that facilitate its regrowth. Consequently, the cartilage present at birth is the same cartilage that remains until death, and no new cartilage can be produced.
Since there is no cure for arthritis, treatment focuses on managing symptoms through medications, weight loss, physical therapy, home exercises, bracing, and injections. The primary objective of treatment is to reduce inflammation in the knee, thereby alleviating pain and swelling.
If non-operative treatment proves ineffective and significantly impacts daily life, such as work, leisure activities, or sleep, surgery may be recommended. This surgery can involve either a partial or a total knee replacement.
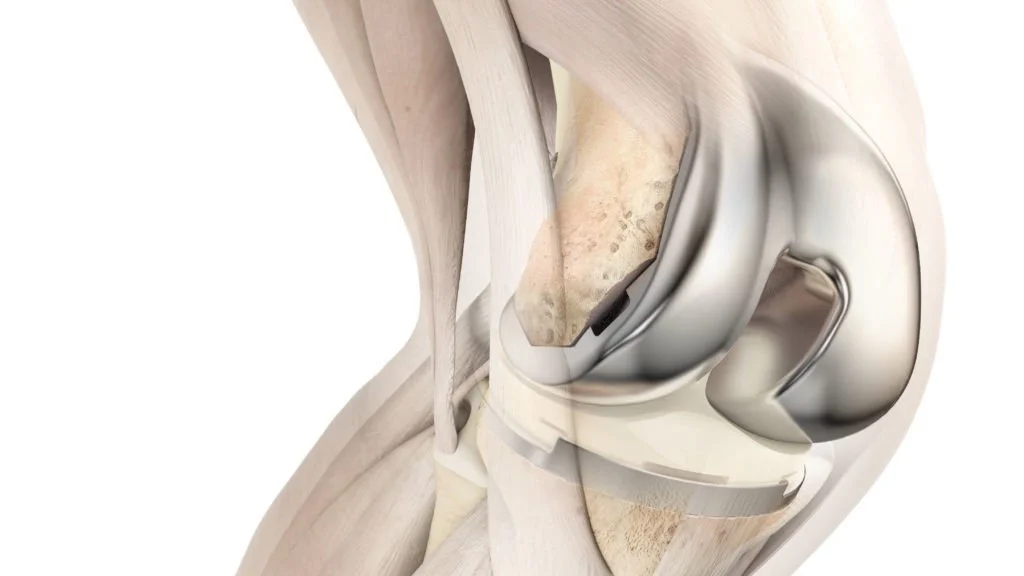
A total knee replacement involves replacing all three compartments of the knee joint: the medial compartment, the lateral compartment, and the patellofemoral joint. In contrast, a partial knee replacement entails replacing only one of these compartments. During the knee replacement procedure, the affected cartilage is trimmed off (approximately 9mm of bone is removed), and metal caps are implanted on both the femoral and tibial sides of the joint. These metal caps articulate with a smooth plastic component (polyethylene) in the center, allowing the knee to glide smoothly. This smooth gliding motion reduces friction within the joint, thereby alleviating pain and swelling and restoring mobility and function.
-
X-ray imaging is the primary diagnostic method employed for osteoarthritis. Other diagnostic modalities include magnetic resonance imaging (MRI) and surgical procedures such as knee arthroscopy. While X-ray imaging may not be infallible, it remains the most accessible and cost-effective diagnostic tool for osteoarthritis.
Bone is the sole human structure that can be distinctly observed on X-rays. Magnetic Resonance Imaging (MRI) is employed to visualize soft tissues such as the meniscus, muscles, and tendons. However, MRI does not provide a clear visualization of bone. Cartilage is not discernible on X-rays and is poorly visualized on MRI. To diagnose arthritis, which is characterized by the degeneration of cartilage, we primarily rely on X-ray findings, which predominantly involve the narrowing of the space between bones. Since cartilage does not appear on X-rays, when the space remains preserved, it suggests that the cartilage is likely healthy. Conversely, when the space narrows, it indicates that the cartilage is deteriorating, exposing the underlying bone (which is indicative of arthritis). Additional signs that are considered include the formation of bone spurs, bone sclerosis (a hardening of the bone), subluxation of the bone, and bone deformities.
-
What is the difference between them?
A partial knee replacement replaces only one of the three compartments of the knee joint, whereas a total knee replacement replaces all three compartments. The knee joint comprises three distinct compartments: the medial compartment (inner portion), the lateral compartment (outer portion), and the patellofemoral compartment (subsequently to the kneecap). A partial knee replacement selectively replaces one of these compartments, leaving the other two intact. Furthermore, a partial knee replacement preserves the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL). In contrast, a total knee replacement replaces all three compartments, including the ACL and PCL.
What is the benefits of one versus the other?
Partial knee replacement offers several advantages over total knee replacement. By replacing only one compartment, the procedure is significantly smaller, resulting in a quicker recovery time of approximately six weeks compared to the twelve weeks required for a total knee replacement. Additionally, partial knee replacement preserves the natural knee structure by avoiding the need to cut the ACL or PCL, which can enhance the overall feel of the knee.
However, partial knee replacement does have some drawbacks. Since only one compartment is replaced, the other two compartments remain exposed to natural wear and tear, potentially accelerating the progression of arthritis and necessitating a second surgery in the future. Nevertheless, it is uncommon for partial knee replacements to be converted into full knee replacements.
Full knee replacement, on the other hand, offers the advantage of replacing all three compartments, eliminating the potential for future arthritis in the affected areas. However, the larger nature of the procedure results in a longer recovery time and may lead to initial stiffness and pain. Furthermore, the removal of the ACL and PCL can impact the natural feel of the knee.
Who is a Candidate for a Partial Knee Replacement?
Individuals with arthritis confined to a single compartment of the knee joint and an intact anterior cruciate ligament (ACL) may be eligible for partial knee replacement. While X-rays are typically sufficient for diagnosing arthritis, they can also be complemented by MRI or sometimes observed during a knee arthroscopy.
What exactly are you doing when you replace my knee??
Many individuals harbor the misconception that we are amputating the distal portion of the thigh bone and replacing it with metal. In reality, we meticulously remove a minimal amount of bone, approximately 9mm from the femoral side and only 4mm from the tibial side. The bone is meticulously trimmed in a specific pattern that facilitates the placement of a smooth metal cap onto the bone. This metal cap is then positioned against a highly polished plastic insert, which significantly reduces friction. Consequently, this reduction in friction leads to a decrease in inflammation, pain, and swelling.
Can you do the “Jiffy Knee”?
“I have heard that the ‘Jiffy Knee’ is the greatest advancement since sliced bread, and I am eager to try it!” When individuals refer to performing the ‘Jiffy’ knee, they are typically describing the approach to the knee joint. While some individuals consider it a groundbreaking innovation, it is also as ancient as sliced bread.
There are multiple approaches to the knee. The most commonly used is what is called the parapatellar approach, meaning it goes around the patella splitting the quadriceps tendon in half. The other approaches are known as ‘quadriceps sparing’ approaches in that they don’t cut the quadriceps tendon. These approaches are the midvastus (cuts through that vastus medialis muscle) and the subvastus (goes below the vastus muscle). All three of these approaches have been done for many years. Different scientific studies will argue there is benefit to doing the quadriceps sparing approach and others say there is no difference. The benefit of the parapatellar is that it allows for a better exposure so your surgeon can see everything whereas the quadriceps sparing approaches have limited exposure.
So in short, there is nothing special about the “Jiffy” knee other than it is a marketing technique to get patients to come to those surgeons that pay money to use that name. I would be happy to use this exposure for you if this is what you would like.
-
How to schedule surgery
Surgery appointments can be scheduled by meeting with Dr. Ward in his office or by contacting the office if you have already met with him. You can leave a message requesting a surgery appointment, and Dr. Ward or his PA will meet with you prior to surgery to answer any additional questions.
Dr. Ward will then place the surgery order, and his surgery scheduler will contact you to provide available dates. You can select the date that best suits your schedule. Dr. Ward performs surgeries at Oro Valley Hospital and Northwest Medical Center, and you can choose either location.
Will my insurance pay for the surgery?
Yes, total knee replacement is an elective surgery although it is considered a medical necessity when you have failed non-operative treatment and insurance will therefore pay for the surgery. How much of the surgery they will pay for depends on your plan and deductible. Contacting your insurance company directly is the best way to know how much it will cost you. Dr. Ward’s office will work with the insurance company to make sure that you are pre-approved for surgery prior to your surgery.
Preoperative Testing
Because knee replacement is a bigger elective procedure we want to make sure that you are as healthy as possible and reduce the chance of complications. We will obtain routine preoperative work up to make sure you’re healthy.
Orders will be generally be given to you at your preoperative appointment. You can get the testing done at Oro Valley Hospital or Northwest Hospital and no appointment is necessary.
Medical Clearance
If you have advanced lung, heart, or kidney problems it is recommended that you get a medical clearance from your primary care provider. It is not needed for high cholesterol or stable high blood pressure. Primary care offices are familiar with these requests and can often be done over the phone or they may ask to see you in the clinic. Your primary care provider will then send a letter to Dr. Ward.
If you see a cardiologist, the anesthesiologist will require you get a clearance from them prior to your surgery.
Preoperative Appointments
Prior to surgery, Dr. Ward or one of his PA’s would like to meet with you one last time to give you your preoperative orders and answer your questions (write them down!), and review the plan for surgery.
Also during this appointment we will review which pain medication plan works best for you and give you a referral for physical therapy. If you need a prescription for a walker we can give it to you at this time as well but most people will either borrow one or get one from a thrift store.
Physical therapy
Schedule physical therapy to start approximately 7-10 days after your surgery. This will give some time for your knee to heal and for the inflammation to calm down. Dr. Ward will also give you some exercises to start at home prior to seeing physical therapy.
Home Medications
Most home medications can be taken all the way up to the day of surgery. Stop all medications the day of surgery other than heart medications.
Stop aspirin 7 days prior to surgery
If you are on blood thinner medication this will need to be stopped with the guidance of your primary care or cardiologist. Please inquire of when they would like you to stop taking your blood thinner medication. They are typically stopped about three days prior to your surgery.
You may restart your blood thinner medication the evening of the day after your surgery.
Time of Surgery
We will try to give you a surgery time when you book your surgery. Unfortunately there is a possibility that your time may change. The OR will call you the day before (Friday if your surgery is on Monday) to confirm the time of your surgery and the time you need to arrive. Times may change due to equipment arrangements or for efficiency in the OR.
Eating Before Surgery
You are not allowed to eat anything at all 8 hours prior to surgery. Because surgery times can vary slightly we recommend that you eat nothing after midnight prior to your surgery.
If you eat after this time the anesthesiologist will cancel your surgery!
If you need to take medications the morning of surgery you may take a small sip of water only to help it down. You may also wet your mouth if your mouth is dry but do not drink it. Food or water in your stomach risks the possibility of it coming up during surgery and going into your lungs which can make you seriously ill.
Skin preparation
Special soap is not needed prior to surgery. It is recommended that you shower the morning of surgery with regular over the counter soap.
Stop applying lotion to your legs the day before surgery.
Do not shave your legs for 2 days prior to surgery if you use a blade. You may shave the day before you if you use clippers.
Medication Prescription
Dr. Ward will try to prescribe your post operative medication prior to surgery at your preoperative appointment or one to two days prior to your surgery. If it is not done at that time then it will be done on the day of your surgery.
Exercise
Exercising, up to the day before your surgery, helps improve your strength, range of motion and endurance. This helps lead to a successful outcome and quicker recovery.
Dr. Ward recommends no impact aerobic exercises. Bicycle, elliptical, and water exercises are all great exercises to do prior to surgery. Focus on building your thigh muscles, this will have a significant impact on your post operative recovery!
Diet and Nutrition
Healthy eating and proper nutrition before your surgery aids the healing process.
Drink plenty of fluids and stay hydrated.
Eat more fiber to help avoid constipation (often caused by pain medications). Foods that contain fiber include corn, peas, beans, avocados, whole wheat pasta and breads, broccoli, and almonds.
Eat foods rich in iron, such as lean red meat, dark green leafy vegetables, raisins, and prunes.
Eat foods high in Vitamin C to help your body absorb iron. Foods that are high in vitamin C include oranges, cantaloupe, and tomatoes.
Make sure you are getting enough calcium, which is needed to keep your bones strong. Foods that are high in calcium include milk, cheese, yogurt, dark leafy greens, and fortified cereal.
Smoking and Alcohol Use
Smoking - Smoking causes breathing problems, increases the risk of medical complications, and slows recovery. Smoking also increases the risk of infection and blood clots after surgery. If you smoke, we encourage you to quit at least a few weeks before surgery.
Alcohol Use - Encourage alcohol reduction prior to surgery. Following surgery drinking alcohol while taking pain medication can result in dangerous side affects including slowed breathing and poor balance.
Diabetes Guidelines and Blood Glucose Management
Managing your blood glucose is always important, but it is extremely important before surgery. In fact, managing your blood glucose before surgery can help reduce the risk of problems after surgery, such as infection and other complications. Surgery can affect your blood glucose control in many ways. Stress before and after surgery can cause your body to release hormones that may make it more difficult to manage blood glucose levels. Surgery can also affect your normal diet, and may change your usual medication routine.
Home Safety Preparation
Setting up your home for your return before you have surgery will help keep you safe, make your life easier, and aid in your recovery. Listed below are suggestions for preparing your home for a safe recovery.
Move obstacles – such as throw rugs, extension cords, and footstools – out of your walk way. Create a wide, clear path from your bedroom to your bathroom and kitchen so you can easily move about with a walker.
Bathroom
You may choose to have an elevated toilet seat or commode and a shower chair but it is not required. Move obstacle so you can get your walker into the bathroom.
Sitting
Sit in chairs that keep your knees straight with no cushion underneath your knee. Sitting with your knee straight is imperative to a successful outcome. A straight knee is needed to walk without a limp. A recliner does not allow for your knee to be straight unless your prop it up to allow your knee to be completely straight with nothing but air underneath your knee.
Access to Items
To avoid reaching or bending, keep frequently used items within easy reach, especially in the kitchen, bathroom, and bedroom. It’s a good idea to carry a cell phone or portable phone with you at all times during your recovery.
Stair climbing
It’s okay to climb stairs without assistance, if you are able. However, you may need help with climbing stairs when you first get home. Consider installing handrails or make sure existing handrails are secure. When going up the stairs lead with your good leg and when going down lead with your bad leg.
Laundry and dining
Get help with cleaning and laundry. Have a few weeks’ of clean clothes available.
Arrange for help with your meals and perishable foods (milk, salad, and fruits and vegetables). Freeze pre-made dinners before your surgery. Stock up on non-perishable foods (boxed, canned, and frozen) to make it easier to prepare meals after surgery.
Driving
Arrange for someone to drive you to your after surgery appointments. Absolutely do not drive while taking narcotic medications. Do not drive until you have regained the range of motion, strength, and reaction time needed to drive safely. If you had your left knee replaced then you may drive when you are not taking narcotics for four hours prior to driving. If you had your right knee replaced then you must be off of a walker and be able to place all of your weight through your leg without an assistive device. You need to be able to slam on the brake peddle in case of an emergency.
-
Reminder
Do not eat anything after midnight the night before your surgery (your surgery will be cancelled if you eat!!)
Have a good night sleep prior to surgery (and so will Dr. Ward!)
Do not take your regular medication except cardiac medications with only a small sip of water.
Take a shower with soap that does not have lotion in it.
Arrive to the hospital in comfortable clothes
Things to bring with you to the hospital
Comfortable clothes and shoes to easily change back into after surgery
Cell phone
Identification and insurance card
Someone to drop you off and pick you up after surgery
Be prepared to remove dentures prior to surgery
Glasses (do not wear contacts to surgery)
Things NOT to bring to the hospital
Walker (have it available to use when you get home)
Ice machine
Jewelry (remove all rings and piercings if able)
Medications
Makeup
Arrival
Arrive at your scheduled time and check in at the surgical receptionist desk. They will then take you back to the preoperative area where the nurse will start your IV and get you ready for surgery. Dr. Ward will meet you there as well as the anesthesiologist. Any remaining questions will be answered at that time. Your loved one may accompany you in this area.
Anesthesia
The anesthesiologist will talk with you about different options for anesthesia during surgery. The anesthesiologist will help you decide which anesthetic is best for you.
Dr. Ward generally recommends a nerve block prior to surgery followed by a “spinal” (similar to a epidural) which numbs your lower extremities. This allows you to wake up without pain and then we are able to stay ahead of the pain as it slowly comes on. This also requires less anesthesia medication which minimizes side effects of the anesthesia (ie nausea).
Dr. Ward will also inject your knee during surgery with a numbing medication to help with the pain afterwards.
Length of surgery
The actual length of the surgery takes on average 60-90 minutes. It takes roughly 15-20 minutes to get you into the room and to put you to sleep. You are then taken to the recovery room for 45 minutes after the surgery.
Dr. Ward will call your family or friend that you designate as your contact directly after the surgery to update how it went! Dr. Ward may also see you in the recovery room but because of medication it is common to forget this part.
After you leave the recovery room you will go to the “Phase two” area where you will work with the nurses to get up out of bed, make sure you are not nauseated, and are safe to go home. This generally takes 2-4 hours depending on the person.
If you are scheduled to stay in the hospital over night then you will go directly to your room following the recovery room. You will participate in physical therapy in your room and will be required to be cleared by them prior to being discharged home.
Incision
Your incision will extend from two finger breaths above your knee cap down to the tibial tubercle.
Your incision will be closed with sutures under your skin that are absorbable and will not need to be taken out.
It will be dressed with an ace bandage that you will leave on for 2 days to help with swelling. Under the ace is a adhesive bandage (Mepilex dressing) that will stay on for 7 days. Do not get it wet. And underneath that is a “Prineo” (mesh type) dressing that is glued to the skin and will stay on for about two-to-three weeks. This can get wet with normal showers but do not soak it under water. It will slowly start peeling and you can trim it as it peels off or pull it off at around 3 weeks.
Recovery Room
Following surgery you will be taken to the recovery room where you will wake up from surgery. Dr. Ward will say hi to you and let you know how it went if you are awake. Because of the anesthesia it is common to forget things during this time. Dr. Ward will call your family or friend to let them know how surgery went. You are generally in the recovery room for 45-60 minutes.
Phase Two
If you are planning to go home after surgery you will go to what is called phase two recovery. Here you will work with the nurses and physical therapy to make sure that you are doing well enough to get out of bed safely and are feeling well enough to go home. Occasionally some people don’t quite feel they are able to go home and the nurses recommend staying one night in the hospital during this time. You are generally in phase two area for 2-4 hours.
-
Blood Clots
It is uncommon to get a blood clot after surgery but you are at increased risk following surgery. Injury to the leg (surgery) induces clotting cascade to stop the bleeding which increases risk of blood clotting in the veins. Another risk factor is not moving as much after surgery which results in pooling of the blood.
To prevent blood clots Dr. Ward will put you on a blood thinner temporary for the first 14 days. For those that are not already on a blood thinner a simple baby aspirin (81mg) twice a day is good enough. If you were on a blood thinner prior to surgery then you may restart your blood thinner the evening on the day after surgery.
The best way to prevent blood clots is movement! When your calf muscles contract they squeeze the blood in your lower legs which helps move the blood back to your heart. This helps reduce the risk of blood clots and helps reduce swelling. Simply pumping your ankles while resting will help reduce swelling and blood clots!
Pain after surgery
Unfortunately pain is unavoidable but we want to make it as tolerable as possible. Stay ahead of your pain during the first 3 days of surgery and then you may start to back off. Trying to catch up on your pain if you get behind is very difficult and can become very uncomfortable!
The sharp pain will decrease after the first week or two although not completely resolve. It is common to have discomfort at night like a tooth ache for about the first six weeks. Continuing to take anti-inflammatory medications will help decrease this.
Ice is one of the best things you can do to help decrease your pain in your knee. It is a excellent pain killer and also helps decrease swelling which will help with your range of motion and decrease the feeling of tightness.
Nausea
It is common to have some nausea after surgery due to the anesthesia and pain medication. Dr. Ward will prescribe you some nausea medication to help in the early days. Constipation can also cause nausea. A cool compress, fan in your face, and walking around can help decrease nausea.
Constipation
Constipation is a common side effect of pain medication. Reducing pain medication as you are able to tolerate will help reduce constipation. Walking is one of the best ways to get your bowel moving (just like your dog). High fiber diets with plenty of water also aids it gut mobility. Dr. Ward will also prescribe Docusate medication which is a stool softener. Take this medication as you need it after surgery. If you continue to have constipation that does not seem to be resolving then try Miralax which is a bowel stimulant. Just be cautious that once the “dam” breaks then things will continue to flow!
Urinary Changes
If you had a spinal anesthesia for your surgery there is a possibility that you can have temporary changes in your urination. The spinal anesthesia may temporarily paralyze your bladder leading to difficulty urinating. In males this may lead to inability to urinate and in females this may result in overflow incontinence. The effects usually only last 1-3 hours but may last longer. It is generally required to urinate prior to discharge home. If you notice inability to urinate for greater then 8 hours then it is recommended to go to the ER to be evaluated.
It is also possible to experience increased need to urinate for the first couple days following surgery. This may be due to the fluid that is administered during surgery and your temporary water retention after surgery. This is generally temporary although can cause urgent need to use the restroom. Being mindful to frequently empty your bladder is recommended.
Medication Refills
Dr. Ward is happy to refill your medication as you need it. There are strict laws with prescribing pain medication and so Dr. Ward is only able to do so much at a time. Please let the office know 1-2 days before you anticipate needing it. We don’t refill medications on the weekend so be sure to plan ahead!
Bruising and Swelling
It is common to have bruising around the knee and may even extend down to the ankle. This varies with people but is nothing to worry about and will resolve after a week or so.
It is also common to have swelling in your knee that extends down to your foot. This will improve with time. You can decrease the swelling by icing it 30-45 min every hour while resting, wearing compression stockings as able, elevating your foot above your knee and your knee above your hip, and pumping your ankle.
Physical Therapy
Physical therapy is a crucial part of your recovery. Regaining your range of motion is the most critical aspect of minimizing pain and allowing you to return to full activity. The physical therapist will periodically measure your motion as well as Dr. Ward. Obtaining full extension is just as important as gaining flexion. This is best done by while sitting keeping your toes pointed toward the sky and allowing your knee to fully extend by not putting a pillow or cushion (recliner) underneath. This will allow gravity to help extend your knee. You can assist it by putting weight on front of your knee.
You will typically participate in physical therapy for roughly three months.
-
What is the my knee replacement made of?
Dr. Ward uses Depuy Attune total knee system. It is made of a alloy metal consisting of cobalt, chromium, and molybdenum metals mixed together. The femoral and tibia component are the metal pieces and between them is a plastic piece called highly crossed-linked polyethylene.
Will I have an issue going through security at the airport?
It depends. A lot of the newer x-ray devices do not set it off but every airport will be different. It is not necessary to have a card to go through security. You should not have to show them your scar. Plan ahead and anticipate that you may need to be further evaluated by the security officer.
I have a pimple like abscess on my incision
Nothing to worry about! This is called a suture abscess and occurs because the body is trying to break down the suture under your skin and sometimes it will form a little abscess. No need to go on antibiotics for it. You can pop it like a pimple if you’d like or let Dr. Ward know at the next visit.
I see a small suture coming out of my incision
This happens occasionally. It’s called suture spitting and occurs when your body tries to reject the suture. It might look like fishing wire is coming out. You can clip it with finger nail clippers or if leave it alone and it will eventually fall out on its own.
My knee is a little warm and red
That is a normal part of healing. You will have increased blood flow to your knee as it tries to heal which will cause increased warmth and a little redness. That is normal to have that for up to three months. It will decrease with time and is usually nothing to worry about.
It’s been 6 weeks and my knee still aches
That is very common. As your knee heals you will continue to work with physical therapy on your range of motion. This causes the scar tissue to release and stretch out. This will cause an ache in your knee for up to around three months. The quicker you achieve your full motion the quicker this will go away.
How long is it normal to be taking pain medication?
Everyone is different when it comes to their pain tolerance and the amount and length of pain medication will be adjusted to each person. It is impossible to have a knee replacement and not to experience pain but our goal is to make it manageable pain. This is done many different ways including medication, ice, improving range of motion, and other modalities.
Getting off narcotics as soon as possible is always our goal to reduce side effects from them and decrease chance of dependence. It is typical to need pain medication for the first two weeks fairly regularly but then that need should decease to only taking it around physical therapy and at night to help you sleep. Ideally by 4 weeks from surgery you should only need a pain pill rarely and then by 6 weeks you should ideally only be taking ibuprofen and Tylenol for your pain. The quicker you get your range of motion back the quicker the swelling and pain will go away. Long term pain and swelling is often due to poor range of motion!
When can I drive?
If you had your right knee done then it is advisable to not drive until you are off the walker and only using a cane for balance. You need to be confident about your ability to slam on the brakes in case of an emergency. If it is your left knee then you can usually drive much sooner but a reminder that you cannot drive while taking pain medication!
When should I be worried?
The biggest things to worry about are the possibility of infection. Sometimes its hard to tell the difference between normal healing and infection. If you have any concerns Dr. Ward would like to see you in the office to make sure its not infected and to give you piece of mind. Don’t ever feel like your wasting Dr. Ward’s time! He would rather reassure you that everything is normal then for an infection to go untreated!
When can I go back to work?
General minimum time off for people that work at a desk is two weeks and for someone that is on their feet to return at 4 weeks. That being said, most people are more comfortable going back to work at 4 weeks for office jobs and 6 weeks for standing jobs.
When can I have my other knee done?
Because you rely on your other side of your body to support you while you are healing Dr. Ward generally recommends waiting until the three month mark to have the other side done.
Do I need antibiotics for dental procedures?
Yes and No. This is controversial and many doctors have differing opinions. Because an infection in your knee is a major catastrophic and life changing event, Dr. Ward recommends that you take antibiotics before invasive dental procedures that may cause bleeding. For general cleaning it is not necessary to take antibiotics. Some dentist offices will provide antibiotics or feel free to call Dr. Ward and he will put some in for you.
Why does my other knee or hip hurt now?
Because you are favoring your surgical knee your other joints will hurt more then usual. As you start walking more normal then this pain should usually return to normal.
Is my leg longer?
No, well yes, well kind of. Let me explain….The biggest reason your leg may feel longer is because prior to surgery you were “bow legged” or “knocked kneed” and now your leg is straight which will make it feel longer. During surgery we typically resect off 9mm off of the femur and about 3mm off the tibia and replace it with the same amount of metal and plastic. Occasionally we have to put a little thicker “poly” (plastic piece) in to make your knee stable but the increase in length is only a couple millimeters and usually not noticeable.
Do I need compression stockings?
Compression stockings can help reduce swelling which can also help reduce some discomfort. Unfortunately they can be difficult to put on and are often too tight at the top and may even make things worse. If you find they are too difficult to put on or do not tolerate them then Dr. Ward is ok with you not wearing them.
Why does my knee make a clicking noise?
Your new knee replacement is made out of metal and plastic. The metal is next to the bone and there is a plastic spacer between the femur and tibia as well as the femur and knee cap. As your knee moves naturally the metal parts of your knee replacement will come in contact with the plastic pieces. This will make a clicking sensation and you may even hear it. This is normal and nothing to worry about. It will be much more noticeable at the beginning but as you develop scar tissue in your knee the sensation and noise will dampen and be unnoticeable for the most part.
My knee is swollen and feels very tight!
This is expected and will resolve with time. Everyone has a different amount of swelling in the knee but the worse of it is for the first two weeks and then slowly subsides. Swelling is a normal part of the healing process and the swelling will even extend all the way down to your foot. Although it is normal for swelling to occur, we want to minimize it as much as possible to decrease your discomfort and allow you to start bending your knee. To help decrease swelling it is recommended you ice your knee 30-45 minutes every hour while resting, take anti-inflammatory medications, wear compression stockings if able, elevate your leg, and pump your ankle. As your swelling decreases it will be allow you to bend your knee much easier.
I have numbness on the outside of my knee!
This is expected and occurs with every knee replacement or surgery that involves an incision down the middle of the knee. The nerve that is in charge of providing sensation to the outside part of the knee is called the ‘infra patellar branch of the saphenous nerve’ and it courses in a horizontal fashion underneath the knee cap from the inside part of the knee to the outside part of the knee. Unfortunately it is impossible to avoid cutting this nerve when making the skin incision. This will result in numbness on the outside part of the knee that may or may not improve with time. In many people it will shrink slowly in size but may be permanent in some people.